The first hours after someone stops or sharply reduces alcohol can be difficult to predict. Families searching for the best nasha mukti kendra in Titwala should look beyond location or labels and ask whether the setting can assess withdrawal risk, monitor changing symptoms and arrange urgent hospital care when needed.
An alcohol withdrawal timeline can explain the usual pattern, but it cannot predict what will happen to one person. Some people develop shaking, sweating or anxiety within hours. Others seem stable at first and later experience seizures, hallucinations or severe confusion.
Withdrawal is more likely after the brain and body have adapted to regular heavy drinking. When alcohol levels fall, the nervous system can become overactive. Previous withdrawal, physical illness, pregnancy, older age, poor nutrition and the use of sedatives or other substances can change the risk.
This article explains what can happen from the first six hours through the third day and beyond. It is an educational guide, not a home detoxification schedule.
Seek urgent medical assistance for these signs
Do not wait for the next stage of a timeline if any of the following occurs:
- Any seizure
- Hallucinations
- Severe confusion or disorientation
- Loss of consciousness
- Breathing difficulty
- Chest pain
- Violent behaviour or an inability to remain safe
- Suspected overdose
- Thoughts of suicide or self-harm
After any seizure, urgent medical assessment and monitored observation are required. The person should not simply be left to sleep at home.
Part 3 of the alcohol education series
This is Part 3 of our alcohol topical authority series.
Part 1, Alcohol Dependence Explained: Symptoms, Withdrawal, Treatment and Long-Term Recovery, explains how dependence develops, what families may notice, why withdrawal can be dangerous and why detoxification is only one part of care.
Part 2, Alcohol Use Disorder: How Doctors Assess Severity and Treatment Needs, covers screening, diagnosis, withdrawal risk, physical and mental health, and the choice between outpatient, residential and hospital care.
This third article focuses on timing. It explains the usual course of alcohol withdrawal symptoms without treating the clock as a guarantee of safety.
The timeline is a guide, not a fixed countdown
People often search for an alcohol withdrawal symptoms timeline because they want to know what will happen next. The concern is understandable. A person may be shaking but still talking normally, or may appear well several hours after the last drink. Families want to know whether the condition is likely to settle or become dangerous.
There is no single answer.
Timing is usually counted from the last drink or from a major reduction in alcohol use. In practice, that starting point is not always clear. Someone may continue taking small amounts, forget when the last drink occurred or use another substance that changes how symptoms appear.
The American Society of Addiction Medicine notes that early symptoms commonly begin within about 6 to 24 hours after alcohol is stopped or significantly reduced. Withdrawal seizures often occur within the first 8 to 48 hours, while hallucinations can emerge during the first day. Alcohol withdrawal delirium generally appears later and can begin several days after the last drink.
The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management stresses the importance of clinical assessment and repeated monitoring rather than relying on a clock alone.
A person does not pass through neat alcohol withdrawal stages in the same order as a diagram. Symptoms overlap, and a serious complication can occur without every earlier stage being obvious.
The first 6 hours: the risk may not yet be visible
The first few hours can appear quiet because alcohol may still be present in the bloodstream. This does not confirm that the rest of the withdrawal will remain mild.
Early changes can include tension, restlessness, headache, nausea or a strong urge to drink. Sleep may be difficult even when the person is tired. Some describe a vague sense that something is wrong before clear physical signs develop.
Families sometimes mistake these symptoms for a hangover or ordinary anxiety. A warning sign is that discomfort becomes stronger as alcohol levels fall or improves for a short time after another drink.
Drinking in the morning to control shaking, sweating or fear suggests that the body may have adapted to alcohol. Someone with a past withdrawal seizure or delirium needs assessment even when they appear stable during these early hours.
From 6 to 12 hours: early symptoms often become clearer
When do alcohol withdrawal symptoms start? They commonly become noticeable within 6 to 24 hours, although the exact timing can be hard to establish when the last drink is uncertain or alcohol use has continued.
Tremor may appear when the hands are held out. Sweating, nausea, headache and disturbed sleep are common. The pulse and blood pressure can rise. Light, sound and ordinary activity may feel unusually irritating.
Anxiety during withdrawal can be intense. The person may pace, repeatedly ask for alcohol or struggle to remain still. These symptoms need to be understood in context rather than judged only by appearance.
A person with serious heart disease, pregnancy, poor nutrition or mixed substance use can face greater risk than a simple symptom list suggests. Someone who looks calm may still have a dangerous history, while severe anxiety can also come from another medical or psychiatric condition.
From 12 to 24 hours: hallucinations and seizures become a concern
Alcohol withdrawal hallucinations can begin during the first day. The person may hear voices, see shapes or insects, or feel something moving on the skin. They may still know where they are and understand that something unusual is happening.
Hallucinations are not always the same as delirium. Delirium involves marked confusion, poor awareness and difficulty understanding the surroundings. Both conditions need medical assessment because withdrawal is not the only possible cause.
Head injury, infection, another drug and a separate psychiatric condition can produce similar symptoms.
Alcohol withdrawal seizures can also occur during this period. These are often generalised seizures that involve loss of consciousness and movements of the whole body. A seizure can happen even when earlier symptoms did not look severe.
Any seizure is a medical emergency. ASAM guidance notes that withdrawal seizures generally occur within about 8 to 48 hours and often peak close to 24 hours. The risks of another seizure and progression to delirium are higher after the first event, which is why monitored care is necessary.
Alcohol withdrawal after 24 hours: the course can still change
Some low-risk cases begin improving after the first day. Others remain active or become more serious.
Tremor, sweating, nausea and agitation can continue. Poor food and fluid intake can lead to exhaustion and dehydration. Repeated vomiting raises concern, especially when the person cannot keep fluids down.
Confusion should not be dismissed as a lack of sleep. A person who no longer knows the date, place or people around them requires urgent assessment.
The risk of alcohol withdrawal seizures remains relevant during the second day. A quiet night does not confirm that the danger has passed.
This is why one normal pulse or one calm conversation is not enough. Withdrawal changes over time. Alertness, orientation, hydration, temperature, pulse and blood pressure need to be considered together.
From 24 to 48 hours: monitoring remains important
During this period, common symptoms may begin to ease. In other cases, they continue with little change.
Hallucinations can persist during the second day, although they often settle when withdrawal delirium does not develop. Ongoing or worsening hallucinations require review because another medical or psychiatric cause may be present.
A person needs urgent care if they have had a seizure, cannot drink fluids, become increasingly agitated or start losing awareness of place and time.
The concern is not simply discomfort. Severe alcohol withdrawal syndrome can affect circulation, temperature, judgement and the ability to remain safe.
Home observation is unreliable when family members cannot monitor continuously, do not recognise changes or live far from emergency services. Continuing to drink small amounts to suppress symptoms also makes the alcohol detox timeline harder to understand.
From 48 to 72 hours and beyond: severe withdrawal can appear later
Delirium tremens is an older term for severe alcohol withdrawal delirium. It is a medical emergency.
The person becomes confused and disoriented. They may not recognise familiar people or understand where they are. Severe agitation, hallucinations, heavy sweating, fever, a very fast pulse and unstable blood pressure can occur.
Alcohol withdrawal delirium often appears later than early tremor, nausea and anxiety. It can begin after the first day and may develop several days after the last drink. Reaching 72 hours does not confirm that the risk has passed.
The timing varies enough that families should not compare the person with a strict online chart. Worsening confusion, collapse, breathing difficulty, loss of consciousness or violent behaviour needs urgent medical assistance at any time.
Trying to restrain the person without trained help can place everyone at risk. Giving sleeping tablets or medicines borrowed from someone else can also worsen breathing, alertness and confusion.
Why withdrawal differs from one person to another
The question “How long does alcohol withdrawal last?” cannot be answered from drink count alone.
The duration and severity depend on the pattern of alcohol use. Someone who has consumed alcohol throughout the day for a prolonged period may have a different course from a person whose heavy drinking is less regular.
Past withdrawal is one of the most useful warning signs. Previous seizures or delirium increase concern. Repeated withdrawal episodes can also make later episodes more difficult.
Risk can rise with serious medical illness, age above 65 and dependence on sedative medicines. Marked signs of nervous-system overactivity, such as a very fast pulse, heavy sweating, raised blood pressure or fever, also require close attention.
Pregnancy can change how and where withdrawal is managed. Poor nutrition, repeated vomiting and dehydration may make the body less able to cope.
Sedatives, sleeping medicines and opioids can alter intoxication and withdrawal. Head injury, low blood sugar, infection, liver-related illness and psychiatric conditions can imitate or worsen the same signs.
Withdrawal is not the same as a hangover
A hangover usually follows a period of drinking and can include headache, thirst, nausea, tiredness and sensitivity to light. It often improves as the body recovers.
Alcohol withdrawal syndrome develops after the body has adapted to regular alcohol use and alcohol levels then fall. Tremor, sweating, marked anxiety, a fast pulse, hallucinations, seizures and delirium point towards a different and potentially dangerous process.
There can be overlap, particularly during the early hours. Morning drinking to control symptoms, a previous history of withdrawal or discomfort that improves after alcohol deserves careful assessment.
Not every shaking hand or confused state in a person who drinks is caused by withdrawal. A doctor may need to rule out low blood sugar, infection, head injury, medication effects and other illnesses.
Who is more likely to need medically supervised withdrawal
A previous withdrawal seizure or delirium places someone in a higher-risk group. Several past withdrawal episodes also increase concern.
Serious heart, liver, kidney or neurological illness can change the treatment setting. Pregnancy, older age, poor nutrition and repeated vomiting require closer review.
Mental health is equally important. Thoughts of self-harm, psychosis, violent behaviour and severe confusion can make home management unsafe.
The home setting also affects the decision. Outpatient alcohol withdrawal treatment may not be suitable when:
- There is no reliable support
- The person cannot return for frequent review
- Emergency services are difficult to reach
- Alcohol or other substances remain freely available
- Violence or severe conflict is present
- The person cannot understand or follow safety instructions
A low symptom score at one moment does not cancel a dangerous history. Withdrawal scales mainly help clinicians monitor current symptoms. They do not replace medical history and clinical judgement when predicting severe or complicated withdrawal.
What medically supervised alcohol detox can involve
Medically supervised alcohol detox begins with an assessment rather than a fixed medicine schedule.
The clinical team reviews the drinking pattern, time of the last drink and previous attempts to stop. Past seizures, hallucinations and delirium are especially important.
Current medicines and other substances must be disclosed. Alcohol combined with opioids, sedatives or sleeping medicines can cause dangerous drowsiness, reduced alertness and slowed breathing.
Pulse, blood pressure, temperature, hydration, alertness and orientation may be monitored. A withdrawal rating scale can help track symptoms once they have started.
Treatment is selected according to the individual’s risk and condition. Fluids, nutrition and related medical problems may also need attention.
Medicine names, doses and home schedules are not provided here because copying another person’s withdrawal plan can be dangerous.
Detoxification manages withdrawal and early physical stability. It does not treat the complete alcohol use disorder. Cravings, mood, sleep, relationships and the risk of returning to drinking may still need care after withdrawal settles.
How long does alcohol detox take?
The phrase “alcohol detox” can mean different things.
Some people mean the period of acute withdrawal. Others mean the full length of time spent in supervised withdrawal care.
Mild symptoms can begin settling after the first day or two. More serious symptoms may continue longer. Delirium can also begin after the 72-hour period shown in many online charts.
Sleep disturbance, anxiety and fatigue often last beyond the most active physical phase. Their presence does not always mean that severe withdrawal is continuing, but they still need attention when they affect safety or increase the urge to drink.
Medical stability, discharge from withdrawal care and recovery from alcohol dependence are three separate milestones. A person should not leave care merely because a fixed number of hours has passed.
Why stopping suddenly without assessment can be unsafe
Not everyone who reduces alcohol will develop seizures or delirium. The problem is that families cannot reliably predict who will.
Online plans often assume the person is otherwise healthy, has never experienced complicated withdrawal and is not using sedatives or other substances. Real cases are rarely that simple.
Trying to control symptoms with alcohol can delay proper care and make the starting point unclear. Sleeping tablets or borrowed medicines can cause additional risks, particularly when mixed with alcohol.
Morning drinking, shaking when alcohol is delayed, previous seizures, hallucinations, severe illness or repeated failed attempts to stop are reasons for medical assessment before attempting withdrawal.
Treatment access in India remains limited
The 2019 national substance-use survey estimated that nearly 15% of Indians aged 10 to 75 used alcohol, representing about 16 crore people.
A later National Academy of Medical Sciences report noted that approximately 5.7 crore people experienced alcohol-related problems and around 2.9 crore showed dependence.
The 2024 report also stated that only about one in 38 people with alcohol dependence had ever received treatment. It cited an 86.3% treatment gap for alcohol-use disorders from the National Mental Health Survey.
These figures relate to earlier survey periods and should not be treated as exact population counts for 2026. They help explain why withdrawal is sometimes first addressed during a crisis rather than through planned care.
The NAMS task-force report on alcohol and substance-use disorders in India discusses the need for stronger screening, treatment and referral across different levels of the health system.
Practical considerations in Thane and Titwala
For a family in Thane, the key question is not whether a centre advertises “detox”. It is whether the setting can assess withdrawal risk, monitor changing symptoms and arrange hospital transfer when necessary.
Travel affects safety. Someone receiving outpatient care must be able to attend review and reach emergency services quickly if symptoms worsen. A plan that is reasonable close to a hospital may become unsafe when the person is far away.
In Titwala, families should ask how medical assessment takes place before withdrawal begins. They should also understand what happens if a seizure, severe confusion or unstable physical signs develop.
Residential rehabilitation may be considered after medical stability when structure and continuing treatment are required. It should never be treated as a substitute for hospital care during severe alcohol withdrawal symptoms.
What happens after the first 72 hours
Passing 72 hours without a major complication can be reassuring, but it does not end the need for assessment.
Confusion, hallucinations, fever, agitation or unstable physical signs still require medical review. Alcohol withdrawal delirium can appear later than many simplified charts suggest.
Even after acute withdrawal settles, sleep, anxiety and cravings can remain difficult. The person may feel physically better and assume that no further treatment is required.
This is a common gap between detoxification and longer care. Treatment for alcohol use disorder can involve medical review, counselling, mental-health treatment, family involvement and relapse-prevention planning, depending on the individual’s needs.
Frequently asked questions
When do alcohol withdrawal symptoms start?
Symptoms commonly begin around 6 to 24 hours after alcohol is stopped or significantly reduced. The exact timing may be difficult to establish when the last drink is uncertain or alcohol use has continued. Drinking history, previous withdrawal, physical health and other substances also affect the course.
What are the first signs of alcohol withdrawal?
Early signs can include shaking, sweating, anxiety, nausea, headache, poor appetite, disturbed sleep and a faster pulse. These symptoms overlap with other conditions. Morning drinking to relieve them, a previous seizure or worsening confusion increases concern.
Can a seizure occur without severe warning symptoms?
Yes. Alcohol withdrawal seizures can happen even when earlier symptoms did not appear dramatic. They commonly occur within the first 8 to 48 hours. Any seizure requires urgent medical assessment and monitored observation.
Are hallucinations always delirium tremens?
No. Hallucinations can occur while someone remains aware of their surroundings. Delirium involves marked confusion and disorientation. Both require medical assessment because withdrawal, other substances and medical or psychiatric illness can produce similar signs.
Does everyone pass through the same alcohol withdrawal stages?
No. The stages shown online are a general teaching model. Symptoms can overlap, develop in a different order or not occur at all. A serious complication can also develop without every earlier stage being obvious.
How long does alcohol withdrawal last?
The most active phase often occurs during the first few days, but duration varies. Severe complications can develop after 72 hours. Sleep disturbance, anxiety and fatigue may continue after the immediate physical danger has settled.
Is an alcohol detox timeline enough to plan withdrawal at home?
No. A timeline cannot assess previous seizures, illness, pregnancy, sedative use, mental-health risks or home safety. Possible physical dependence requires an individual medical risk assessment rather than a standard home schedule.
The clock cannot replace a risk assessment
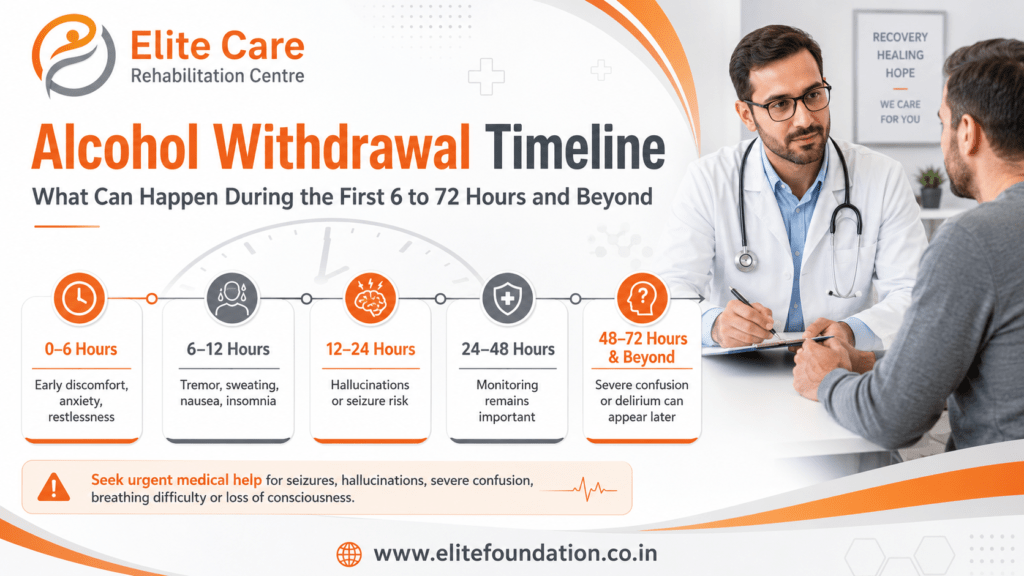
The first 6 to 72 hours can involve mild discomfort, rapid change or a medical emergency. Early symptoms often begin during the first day. Seizures commonly occur within the first two days, while withdrawal delirium can develop later.
These time ranges help explain why monitoring matters. They cannot confirm that withdrawal at home is safe or that the danger has ended after a set number of hours.
The most useful information is the full history: the drinking pattern, last drink, previous withdrawal, current health, other substances and support available. Treatment decisions should follow that risk picture rather than a fixed point on an online chart.
Medical disclaimer: This article provides general educational information and does not replace individual medical assessment, diagnosis or treatment. Alcohol withdrawal can be dangerous. Seek urgent medical assistance for seizures, hallucinations, severe confusion, breathing difficulty, loss of consciousness, chest pain, suspected overdose, violent behaviour or thoughts of self-harm.